[Medicine] - A significant % of the human population suffers
from defective MTHFR genes, which results in elevated Homocysteine
levels, which predicts (ie. may or may not cause, medical evidence
only supports correlation, not causation) significantly increased
risks of cardiovascular disease and strokes. MTHFR gene mutations
also cause significantly decreased Glutathione levels, and is also
strongly linked to at least 60 different medical conditions.
Dr Amy Myers : What is an MTHFR Mutation and What Can We Do
About It?
http://www.amymyersmd.com/2017/07/what-is-an-mthfr-mutation-and-what-to-do-about-it/

Homocysteine and MTHFR Mutations : relation to Thrombosis and
Coronary Artery Disease
http://circ.ahajournals.org/content/111/19/e289
Homocysteine : Associated Diseases, Link to Vitamin Bs,
Homocysteine Reduction Methodologies
http://www.lifeextension.com/Protocols/Heart-Circulatory/Homocysteine-Reduction/Page-02
Methylation and Homocysteine : Factors and Treatment
http://www.foodforthebrain.org/alzheimers-prevention/methylation-and-homocysteine.aspx
--------------------------------------------------------------------------------
Damned if you do, damned if you don't. Welcome to physical
incarnation.
Migraine sufferers have defective MTHFR genes and require High
Vitamin Bs intake to reduce Homocysteine levels to prevent
Migraines
http://articles.mercola.com/sites/articles/archive/2009/04/21/b-vitamins-offer-migraine-relief.aspx
Medical Study finds Link between High Vitamin Bs intake and Lung
Cancer in men
https://sg.yahoo.com/style/study-finds-between-high-vitamin-b-intake-lung-123029252.html
--------------------------------------------------------------------------------
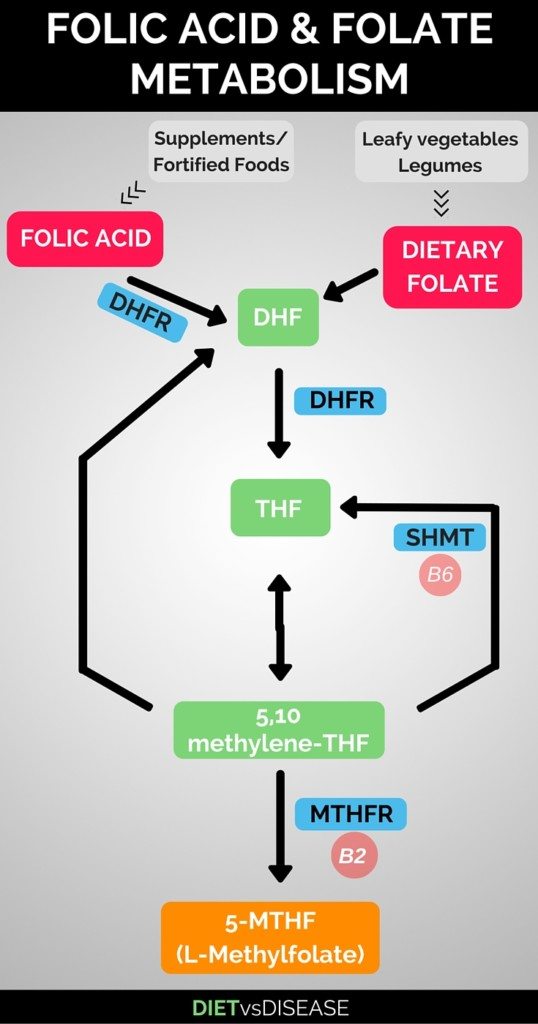
L-Methylfolate (5-MTHF) supplementation required for people who
cannot process folic acid due to MTHFR gene mutation
https://www.dietvsdisease.org/l-methylfolate-5-mthf/
--------------------------------------------------------------------------------

https://en.wikipedia.org/wiki/Levomefolic_acid
--------------------------------------------------------------------------------
Dr Lynch explains why (6S)-5-methyltetrahydrofolic acid is the
correct enantiomer (H2 Chemistry) that is required as
supplementation for sufferers of MTHFR gene mutations :
http://mthfr.net/l-methylfolate-methylfolate-5-mthf/2012/04/05/
[Pharmaceutical Chemistry] - Different Types of Methylfolate,
including Metafolin® versus Quatrefolic®
http://www.podiapn.com/
http://methyl-life.com/methylfolate-types/
--------------------------------------------------------------------------------
Question : I was wondering about the connection between MTHFR
and glutathione you mentioned in your video presentation. It seems
to me that if there is a MTHFR defect, resulting in
undermethylation, that should result in increased availability of
homocysteine to be converted to cysteine, and ultimately to
formation of glutathione. Yet you are saying there may be problems
with glutathione production in MTHFR mutations. Can you explain
why? - A fellow medical doctor.
Dr Lynch replies : Great question. Short term, you are
correct. Short term, the increase in CBS enzyme activity should
lead – and does lead – to increased glutathione production. The
problem is, long term, with MTHFR, and oxidative stress, the
glutathione oxidation increases beyond the point of glutathione
production. This is because the traditional transmethylation cycle
(Methionine cycle) and BHMT pathway help produce CoQ10, carnitine,
phosphatidylcholine, creatine, SAMe – all of which are big players
in antioxidant production and mitochondrial function. As those
decline, oxidative stress increases, CBS upregulation is even
higher – and in turn, due to decreased CoQ10, carnitine, creatine,
etc, ammonia levels climb and potentially so does hydrogen sulfide
levels – and the inability for the sulfonation pathway to keep up
with the increased sulfite/sulfide production thus leading to
sulfur sensitivity and molybdenum deficiency. I should also add
that the likelihood of cysteine, glycine and B6 levels declining
are high due to long term oxidative stress. Then – the production
of glutathione is also affected. Not to mention the decline of
vitamin C, selenium and vitamin E which help prevent oxidized
glutathione and help recycle it back into reduced glutathione. I
believe that if we support the levels of CoQ10, carnitine,
creatine, magnesium, phospholipids, molybdenum, decreased sulfur
foods initially – and decreased sulfur supplements – and possibly
increase SAMe right out of the gate – before even supplementing
with glutathione, methylfolate or methylcobalamin, the degree of
improvement should increase quickly. As improvement occurs, then
supporting phase 2 with glutathione, NAC and glycine should further
help. I think now if we support the MTHFR defects this way – by
reducing oxidative stress, improving cell membrane stability and
replenishing mitochondrial and antioxidant levels – our patients
will improve much faster. Then – once those are in play – then
supporting MTHFR for long term natural production and hopefully
removing that initial supplementation. - Dr Lynch - https://seekinghealth.org/resource/podcast-8-mthfr-and-glutathione-production/
See Dr Lynch's "Supplements to Reduce Homocysteine Levels"
http://mthfr.net/comparison-of-homocysteine-support-products/2011/09/13/
--------------------------------------------------------------------------------
MTHFR gene, Homocysteine and Vitamin B12 : A comparison of
different approaches by Dr. Ben Lynch versus Dr. Amy Yasko versus
Dr. James Braly
http://mthfrliving.com/health-tips/supplementing-for-mthfr-b12/